


WITH AN INCREASINGLY AGING population, clinicians need more robust corrective options to increase good visual outcomes to meet today’s lifestyle and visual demands. However, before diving into a discussion of multifocal options for our presbyopic population, it is important to know why and when practitioners pursue specific options. Multifocal contact lenses (MFCLs) and multifocal intraocular lenses (MFIOLs) are challenging to compare because cataract formation and presbyopia are two distinctly different processes occurring in the same structure, the crystalline lens.1 Presbyopes typically have clear optical media barring early cataracts, and they require a dynamic solution for their increasing difficulty with near focusing. Further, patients with advancing cataracts must address reduced contrast sensitivity, color, brightness, and visual acuity, most often in addition to presbyopia. Cataract surgery notably pushes patients into absolute presbyopia.2
Furthermore, correction with MFIOLs occurs behind the pupil, while an MFCL sits on the cornea, which introduces marginal aberrations through the optics of the lens. Light must bend through the contact lens, the tear film, the cornea, and aqueous in the anterior chamber before it ever reaches inside the eye to resolve a target object at any distance, which increases the opportunity for aberrations or distortions to affect vision. Both, however, serve to meet the visual demands of the aging visual system.
Centration, Stability, and Visual Performance
Contact lenses and IOLs both have their advantages and disadvantages. The performance of MFIOLs is more physiologically stable in the eye compared to contact lenses on the eye because a healthy fitting contact lens is designed to move on the eye. An IOL is, however, vulnerable to intraocular tilt. Alternating methods of correction are nearly impossible with MFIOLs, whereas presbyopia-correcting contact lenses have the advantage of being easy to switch, adjust, or abandon altogether.3 Lens design is also an important consideration. Soft multifocal options today are aspheric center-near, aspheric center-distance, or concentric multizone designs. Diffractive IOL designs are pupil independent, with improvements in near vision function and reduced glare and halos. There are increasing options in the contact lens market for pupil-independent designs. This is an important distinction from refractive IOLs, which perform well at intermediate distances but are pupil dependent, and this issue remains among their greatest disadvantages. Both MFCLs and MFIOLs allow for modified monovision as a correction option.
The core issue with all multifocal corrective options is the resultant image quality degradation, loss of contrast sensitivity, and potential for halos and glare. An important consideration with soft contact lenses is the tendency for lenses to displace temporally while the pupil is anatomically nasally displaced. Fortunately, contact lens manufacturers have the option to decenter the optics of contact lenses to better align with the visual axis.
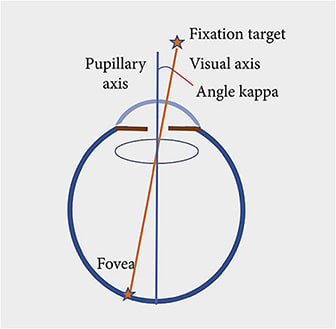
Angle Kappa
Current research suggests angle kappa plays an important role in determining whether multifocal correction is an option for patients.4,5
The ideal location to center a multifocal IOL is between the pupillary center (PC) and the visual axis (first Purkinje image), and the separation of these 2 points is the angle kappa. As with IOLs, we must be aligned as closely as possible to the visual axis with MFCLs. However, we are still limited by our anatomy. There are 2 basic requirements for diffractive optics, which must be met for ideal centration:
- The MFIOL must be lined up so that the rays of light from the cornea converge at the center of and are perpendicular to the lens implant; and
- The lens must be concentric with the aperture, in this case, the pupil5
We cannot satisfy both requirements because the first Purkinje image is almost never centered on the pupil; thus, light scatters more readily, producing the reduction in optical quality (manifesting as glare and loss of contrast sensitivity) observed with MFIOLs. The best that surgeons can do is center the MFIOL somewhere between the PC and the first Purkinje image. Studies have confirmed this concept clinically: patients with a large angle kappa have worse outcomes with MFIOLs than those with smaller angle kappas.6,7 There is a direct relationship between the perception of symptomatic halos and glare and increasing size of the angle kappa, with 0.6 mm representing the cutoff for determining candidacy for an MFIOL.6
It was found that, in an eye with a small angle kappa, rays of light pass through the IOL undisturbed, but in those with a large angle kappa, the rays might hit an edge of the ring of a MFIOL, thus inducing glare and halos.4
Additionally, angle alpha is the difference between the optical center of the cornea and the visual axis.8 If the optical axis and visual axis do not match, as with a large angle alpha, the patient’s visual performance will suffer. A patient whose optical center, pupillary center, and visual axis align as closely as possible will likely have the best postop outcome, and these are measurements routinely collected on devices capable of performing aberrometry and topography, in addition to other types of data collection.
This issue similarly affects patient candidacy for MFCLs. Today, we have the ability to decenter the multifocal optics to better align with the visual axis in patients with a larger kappa. The advantage with MFCLs is that the optical decentration is a far more practical adjustment to make in a contact lens compared to an IOL. Improving centration, whether by decentering the IOL in the bag or decentering the soft MFCL optics, over the line of sight enhances patient outcomes.
IOLs result in an approximately 30% loss of contrast sensitivity and 1 line of acuity loss, and while this tends to be insignificant in terms of visual performance, problems arise when there are noticeable halos or glare in low light levels.6 A good outcome with multifocal correction is that in which the patient tolerates the resultant reduction in acuity and contrast sensitivity. As with MFCL wearers, the IOL must be a good fit for the patient, their visual demands, and their lifestyle choices. Fit the patient, not the lens.
To maximize patient outcomes in multifocal correction, there are a few important considerations, including the optical quality of the visual system prior to intervention.
- Consider advancing cataracts. In patients with markedly reduced best-corrected visual acuity and increasing symptoms of glare secondary to cataracts, contrast sensitivity is also already poor. Any significant improvement post-cataract extraction, even if at the expense of some visual performance, is a successful outcome.
- Optimize the fitting characteristics of contact lenses—stability, centration, healthy movement—and then work on adjusting the power. You do not want a lens that provides optimal visual performance when things are ideal but only works well 60% of the time due to a poor fit.
- Ocular surface disease, dry eye, corneal opacities, and ectasia reduce the potential for good outcomes because we are asking an already sensitive visual system to increase its load with multifocal optics. It is imperative to assess corneal and tear film integrity prior to engaging in an MFCL fitting or when considering MFIOLs, and in many cases, they may be contraindicated.
- In cases of dry eye disease, with improvement and treatment, you may be successful with good visual function using multifocal lenses.
- Patients with macular disease, such as macular degeneration, would do poorly with the loss of contrast sensitivity.9
Patient education is perhaps among the most vital aspects of choosing the ideal candidates for multifocal correction. Clinicians must set proper visual expectations to ensure successful outcomes, and patients must be receptive to the idea that some image quality degradation is a worthy compromise to make to meet their dynamic visual demands. ■

References
- Zimmerman AB, Emch A. Multifocal lenses versus multifocal IOLs. Contact Lens Spectrum, Volume: 27, Issue: August 2012, page(s): 32 – 37.
- Shafer BM, Greenwood M. Presbyopia correction at the time of cataract surgery. Curr Ophthalmol Rep. 2020;8(3):79-87.
- Charman WN. Developments in the correction of presbyopia II: surgical approaches. Ophthalmic Physiol Opt. 2014;34(4):397-426. doi:10.1111/opo.12129.
- Prakash G, Prakash DR, Agarwal A, et al. Predictive factor and kappa angle analysis for visual satisfactions in patients with multifocal IOL implantation. Eye (Lond). 2011;25(9):1187-1193. doi:10.1038/eye.2011.150
- Karhanová M, Marešová K, Pluháĉek F, et al. The importance of angle kappa for centration of multifocal intraocular lenses. Cesk Slov Oftalmol 2013;69:2:64-8.
- Kumar A. Angle kappa may play important role in success of multifocal IOLs. Healio Ophthalmology website. May 10, 2010. Accessed June 6, 2021. http://www.healio.com/news/ophthalmology/20120331/angle-kappa-may-play-important-role-in-success-of-multifocal-iols .
- Karhanová M, Pluháĉek F, Mlĉák P, et al. The importance of angle kappa evaluation for implantation of diffractive multifocal intra-ocular lenses using pseudophakic eye model. Acta Ophthalmol. 2014;93(2):e123-e128. doi:10.1111/aos.12521.
- Devgan U. Angle alpha and angle kappa with IOLs. Cataract Coach website. September 7, 2020. Accessed June 6, 2021. http://cataractcoach.com/2020/10/07/angle-alpha-and-angle-kappa-with-iols/ .
- Holladay JT. Multifocal IOLs: patient selection and optical performance. Healio Ophthalmology website. January 31, 2017. Accessed June 6, 2021. http://www.healio.com/news/ophthalmology/20170125/multifocal-iols-patient-selection-and-optical-performance .

